
Unit 5 Introduction
Substance use is widespread in our society, and teenagers are at the greatest risk for substance use disorders and addiction. This unit focuses on the neurobiology of how reward works in the brain and how drugs can “co-opt” this system as well as affect neurotransmission in the brain. The topics throughout this unit focus on helping students understand the biological risk factors for substance use disorders, the impact of different substances on the brain, and social and medical approaches to prevention and treatment.
Note for teachers: This terminology guide from the National Institutes of Health may be helpful in talking about substance use and addiction while avoiding stigma and negative bias.
What's In This Unit?
- Lesson 1: Substance Use & Disorders
- Lesson 2: Drugs & the Brain
- Lesson 3: Treatment for Addiction & Policy Concerns
Terms & Definitions: Unit 5
- Dopamine – A neurotransmitter that plays many roles in the brain, including an important one in the reward system. Dopamine is released by certain neurons in response to rewarding or motivating stimuli.
- Substance Misuse – Substance use that involves the use of illegal drugs or the inappropriate use of legal substances.
- Drug Tolerance – As the body adapts to the presence of a drug, the same amount produces less of a reaction. Over time, a higher dose has to be taken to achieve the same effect.
- Withdrawal – Negative mental or physical symptoms that result from stopping or reducing the intake of a drug.
- Detoxification – A medical treatment that helps to rid the body of a drug while managing withdrawal symptoms. This is typically thought of as only the first step in treatment, and often not sufficient to break an addiction.
- Relapse – A common condition in which a person begins using a substance again after stopping or reducing use for a period of time.
- Triggers – Internal or external cues, such as objects, situations, or people in a person’s environment, that increase craving for a substance because of learned associations.
Lesson 1: Substance Use and Disorders
Objective: Students will learn about the prevailing theories on what addiction is and why different people may be at different risk for substance use disorders.
ENGAGE/HOOK: Is All Substance Use “Bad”? (10 min)
Introduce the lesson by explaining the background information below and guiding them through the following activity:
This lesson will focus mainly on how different substances affect the brain. Substance use can be a contentious topic, and societal ideas around which drugs are “good” or “bad” have changed throughout history.
Guide students through the activity using the steps below. This activity can be run as a discussion or as a worksheet that students fill out individually:
- Pose these questions to students for an initial discussion, or use the substance use anticipation guide worksheet to have students answer these questions on their own.
- Is all substance use “bad”?
- What about drugs that alter your brain functions? Are all brain altering drugs “bad”?
- Are there certain drugs or certain contexts where use of a brain-altering substance could be considered “good”? How would you decide if a certain type of substance use is “good” or “bad”?
- Ask students to read the article “Can Psychedelics Solve the Youth Mental Health Crisis?” (The Nation) on the use of substances for treatment of certain medical conditions.
- After they read the article and ask the questions above again (or fill out the second column of the worksheet).
- Have their minds changed?
- Do they have new evidence to support their original answers?
EXPLORE: Addiction Card Game (30 min)
Guide students through an addiction card game adapted from the "What's the Deal?" activity from BrainU. Modified directions are below.
The game is modified blackjack where students cannot see their starting card which represents their “risk factor.” In the Launch Lesson, we discussed that both genetics and the environment play a role in shaping our brains, and our risk for addiction is no exception. Thus the “risk factor” in this game includes both genetic and environmental factors.
Materials Required: 1 deck of cards per group of 4.
- Explain to the students that they will be playing blackjack, but with a twist. This game will help us simulate addiction and what can lead to it.
- Explain to students the rules:
- The idea of blackjack is to reach a score closest to, but not over, 21. The player closest to 21 at the end of the round wins. If you go over 21 you are out.
- Face cards are worth 10 pts each and other cards are worth their number value.
- In normal blackjack, each player has a card face down that only they can see. Each player asks the dealer for more cards in order to add their value to their face down card, getting as close to 21 as possible.
- However, in this version of the game there is a twist: the players cannot see their face down card.
- Break students into groups of 4. Assign one student as the dealer and the rest are players.
- Dealer gives each player a card face down. The dealer can look at it but the players cannot!
- Players can then ask the dealer for cards one at a time. These cards are dealt face up.
- When a player thinks they have reached close to 21 they stop asking for more cards.
- At the end of the round each player turns over their face down card and adds up their total including the face down card. The score closest to 21, but not over, wins! If their score is greater than 21 they are out.
- Play a second round following the same rules. If there is time they can play a third round as well.
- Answer the questions below after completing at least two rounds.
- What was your score after the first round? If you went over 21, what led to this outcome?
- What was your score after the second round? Were you more or less risky in the second round? Why?
- Think about this game as an analogy to the risk of developing a substance use disorder.
- What do you think it means to go over 21?
developing an addiction - What do you think the face down card represents?
the combination of your genetic and environmental risk… students may only come up with one but make sure to emphasize that both are important - What do your card selections represent?
your individual choices about behavior
- What do you think it means to go over 21?
- What factors affected your decision making in the game, and how might they translate into real life decision making?
- Can you predict who will go over 21 in the game without seeing their facedown card? How might this shape our thinking around substance use disorders?
EXPLAIN: Substance Use Disorders
The following information is teacher-facing and can be utilized to teach students new information in whatever format works best for you and your students.
Key Points:
- The health impacts of substance use fall along a spectrum. Addiction is one of the most severe types of substance use disorders, when an individual can no longer control the impulse to use a substance even when there are negative consequences.
- People living with substance use disorders have historically faced stigma and discrimination, creating barriers to appropriate treatment and care.
- Genetic and environmental factors can both place some people at greater risk of developing a substance use disorder.
- Misregulation and misuse of legal pain medicines, followed by the increase in illegal opioid substances, have led to a serious public health crisis.
Use vs. Misuse vs. Addiction
The impact of drugs on our health occurs along a spectrum, therefore terminology is important. Substance use refers to any use of selected substances, including alcohol, tobacco products, drugs, inhalants, and other substances whose intake can result in possible dependence and other detrimental effects. Substance misuse encompasses a broad range of behaviors, including overindulgence in alcohol, misuse of prescription medication, or use of illegal drugs. Addiction falls at the most severe end of the continuum of substance use disorders, which are associated with a person’s reduced ability to control their impulse to use drugs even when there are major negative consequences. These distinctions are important because using a particular drug once or twice does not usually lead to a substance use disorder for most individuals. In fact, most drugs have helpful and clinically relevant uses. Similarly, if occasional misuse doesn’t change or interfere with someone’s normal life and activities, it is not an addiction. Addiction is when a substance is misused to the degree that it is relied upon for daily function, interferes with day to day life, and changes the brain so that stopping its use is difficult, both physically and emotionally.
Stigma and Substance Use Disorders
Is addiction a choice, a brain disease, or something that has elements of both? Addiction is a complex mix of biological, psychological, and environmental factors that can be modeled in laboratory animals. However, the everyday experiences of people living with a substance use disorder are more complex than what scientific findings can explain. As our scientific and medical knowledge has progressed, we increasingly approach addiction as a chronic, treatable disease. However, older beliefs about addiction still result in stigma and discrimination today, which can often stand in the way of people accessing and receiving the medical care and treatment they need. Some people find the discussion of addiction as a disease to be stigmatizing in a different way, as the term ‘disease’ paints a picture of permanent ailment that removes a person’s free will, or of a curable condition if the right miracle treatment drug is provided. Although some stigmatizing terms may be used colloquially, modeling the right language in clinical and educational settings is important for respecting people’s identity and dignity.
Genetic & Environmental Risk Factors
What leads to substance use disorders? Many studies show that more than half of a person’s risk is based on genetics, and that this may vary depending on the particular substance. But genes aren’t everything, and factors such as the availability of the drug and a person’s environment may have nearly as large an impact. Chronic stress, especially early in life, is a major risk factor for developing a substance use disorder. Family dynamics, socioeconomic status, and neighborhood or school environments play another large role. And especially in teenagers, who are highly attuned to their peer groups, social environments matter as well. (For more on the increased plasticity of the teenage brain and why teens are at higher risk for becoming addicted to substance use, see Unit 2). Part of the reason that addiction is so hard to treat is that it develops from such a complex mix of influences and varies from individual to individual.
Opioids: A Public Health Crisis
In the late 1990s, new opioid medications for pain were introduced that claimed to provide pain relief for longer periods of time. Aggressive marketing and a lack of regulatory oversight led these drugs to be prescribed at high doses that then wore off more quickly than expected, putting patients at higher risk for addiction. By 2004, OxyContin, the most popular of these drugs, was the most misused drug in the United States. When patients were taken off the drug, many were not able to cope without it and turned to illegal opioids like heroin. Similarly, new and extremely potent opioids such as fentanyl and xylazine were developed and continue to be used as sedatives and painkillers for both human and veterinary medicine, but are now flooding the black market. As a result, the danger of overdose has risen and it is more important than ever that people with substance use disorder are able to be supported as they seek treatment. Since the late 1990s, deaths due to overdose have steadily climbed, reaching new heights during the COVID19 pandemic.
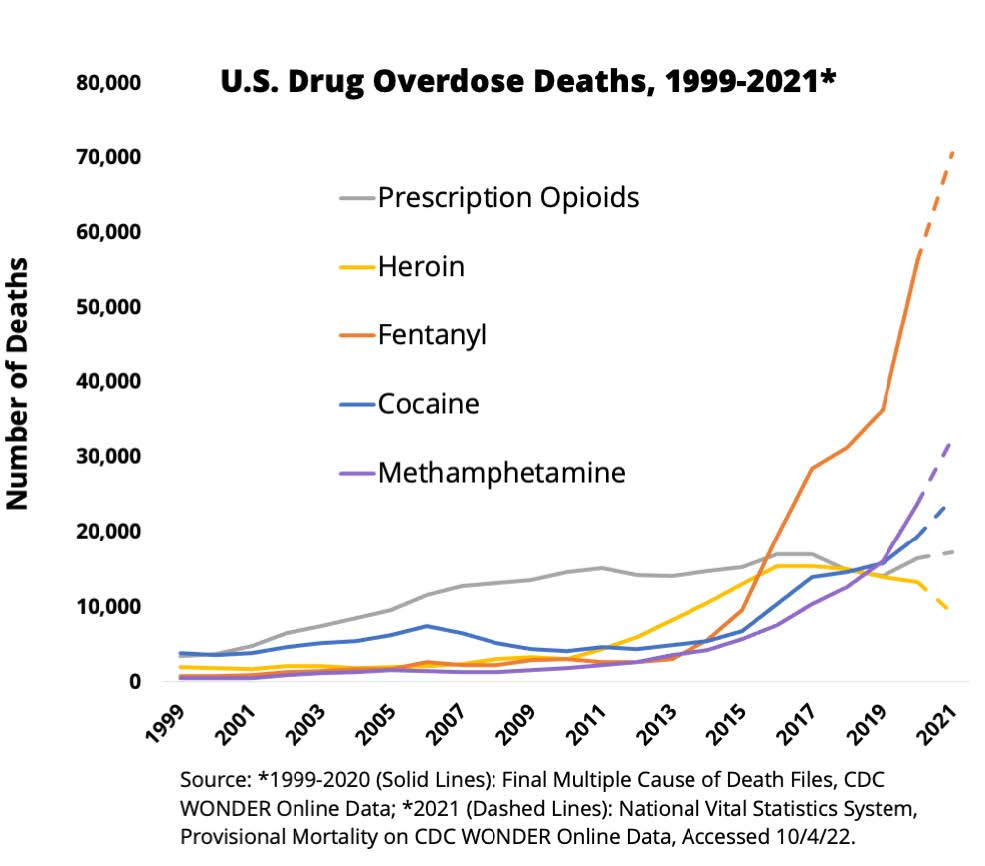
In the early 2000s, the overdose deaths were driven by misuse of prescription opioids, but as regulations around prescription tightened, and more powerful drugs like fentanyl became more common on the black market, this pattern changed, and continues to do so. Image credit: National Institute on Drug Abuse
Additional Resources
- Use vs. Misuse vs. Addiction
- This high level review of addiction addresses substance use and other compulsive behaviors as well as risk factors for addiction. (Psychology Today)
- This video discusses the brain science of addiction, with a focus on the vulnerability of the teenage brain. (The Franklin Institute)
- Families for Addiction Recovery shares personal perspectives from people in recovery from substance use disorders.
- This article compares chemical addiction associated with substance use to behavioral addictions involving compulsive behaviors such as gaming and gambling. (Healthline)
- Stigma and Substance Use Disorders
- A rationale for classifying addiction as a chronic disease by the Partnership to End Addiction.
- Marc Lewis, a neuroscientist in recovery from a substance use disorder , discusses his experiences and his book on how neuroscience should talk about addiction in terms of a learned pattern of behaviors, not as a disease.
- The commentary describes some of the history of the stigma surrounding substance use disorders and addiction and what some non-profit organizations are doing to combat it. (National Academy of Medicine)
- This guide is another resource with practical suggestions on what we can all do to help reduce stigma around substance use disorders. (Johns Hopkins School of Medicine)
- In this article, a journalist recounts his personal experience with stigmatized reactions to his substance abuse disorder. (STAT News)
- Genetic & Environmental Risk Factors
- This resource lists both risk factors and protective factors for youth at high risk for substance use disorders. (Centers for Disease Control and Prevention)
- The Genetics Science Learning Center has short sound bites about environmental risk factors, genetic risk factors, and risks due to the adolescent brain.
- The Turning Point rehabilitation clinic of Tampa has a page about some common environmental risk factors for substance use disorders.
- Opioids: A Public Health Crisis
- This 2022 interview with public health expert Howard Koh provides a brief overview of the causes underlying the opioid epidemic and reasons for optimism. (Harvard School of Public Health)
- This 2009 article gives a thorough history of the marketing and misregulation of OxyContin. (American Journal of Public Health)
- This website charts the different phases of the opioid epidemic and current strategies for response. (Centers for Disease Control and Prevention)
ELABORATE: Ripple Effects (30 min)
Guide students through the following “Ripple Effects” activity developed by the National Institute on Drug Abuse, which looks at the impact drugs may have on individuals and their communities.
Note to teachers: It is common for students to have only considered the impact of using drugs on their own bodies, minds, and lives, but drug misuse and addiction can have widespread impacts. Some teachers may want to complete the Ripple Effects activity on a non-drug example first to get students accustomed to thinking in this way. Possible examples of a non-drug option could include the impact of hunger/food insecurity, owning your own home, or having a chronic illness.
- Print out two copies of the Ripple Effects student worksheet per student pair. (The Ripple Effects teacher guide shows some broad categories of effects that could be explored at each level.)
- Pose the following questions to students and ask them to discuss in pairs prior to completing the worksheet:
- What impact does drug use have on individuals, their families and their communities?
- Have students fill out the Ripple Effects worksheet with their partner: one for marijuana and one from heroin. Give students time to research the effects of each drug at different levels of society.
- Have students discuss with their partners and write the effects they find online into the different spaces on the worksheet.
- Look up the short-term effects of using each drug. Then look up the long-term effects of using each drug.
- Which of each of these effects do you think will impact the individual? Their family? Their broader community?
- Once pairs have completed the worksheet, ask them the following reflection questions:
- Compare and contrast the impacts of marijuana or heroin at each level of society.
- Which drug seems to have the highest negative impact on individuals? Why?
- Which drug seems to have the highest negative impact on the overall community? Why?
- Were you surprised by any of your findings during your research?
- Which communities are most impacted, why? Does the same drug impact all groups/individuals the same way?
Lesson 2: Drugs & The Brain
Objective: Students will learn about the impact of certain drugs on neurotransmission and how some drugs interact with the reward networks in the brain.
ENGAGE/HOOK: Seeing Addiction in the Brain (5 min)
Introduce the lesson by explaining the background information below and guiding them through the following activity:
This activity discusses PET imaging, which is described in greater detail in Unit 3, Lesson 1.
For many individuals who are currently struggling with addiction, there are fewer dopamine receptors in key brain areas of their reward network, which scientists believe is directly related to addiction.
Show students the image below.
The image shows PET scans in which radioactive dopamine is injected to the patient, so we can see where that dopamine binds in the brain. The particular brain region shown in warm colors (which normally has lots of dopamine receptors for the dopamine to bind to) is one of the main reward centers.Image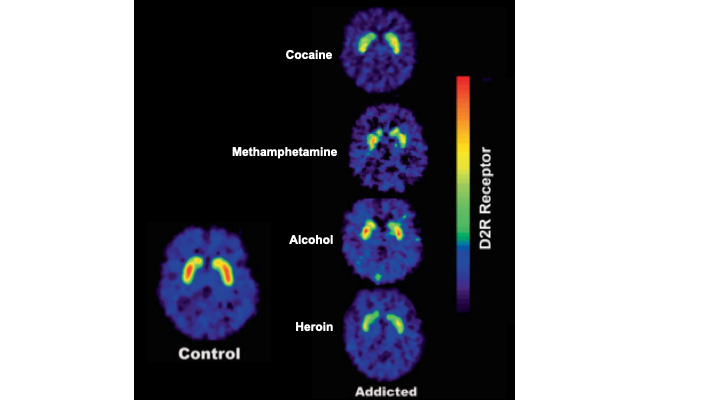
Addiction can have similar impacts on the reward centers of the brain across many different circumstances, compared to controls. Image credit: Adapted from Volkow ND, Fowler JS, Wang GJ, et al. Role of dopamine, the frontal cortex and memory circuits in drug addiction: insight from imaging studies. Neurobiol Learn Mem 2002;78:610–24.
- Ask students to reflect on the following questions:
- What do you notice about the level of dopamine receptors in the control subject (non-addict) vs the subjects with addiction?
Higher than in all subjects with addiction - What do you notice about the dopamine receptors in the brains of patients who are addicted to the four different substances?
They all have lower levels of dopamine receptors - Based on these images, what conclusions can we make about how addiction alters the brain? Does it appear that the substance you are addicted to alters how your dopamine receptors are affected?
It does not appear to matter greatly which of these substances the patient is addicted to, all reduce the number of dopamine receptors compared to control (to slightly different degrees). Mechanisms for addiction to these and more substances are all thought to be similar. - Can we tell from these images whether addiction lowers dopamine receptors OR if people with lower dopamine receptors are more likely to become addicts (causation vs correlation)?
We cannot tell from this data, but we do see the levels of functional dopamine receptors increase in addiction patients who have recovered!
- What do you notice about the level of dopamine receptors in the control subject (non-addict) vs the subjects with addiction?
EXPLORE: Mouse Party (30 min)
Explain the background information below to students to frame the following activity using an interactive online tool for exploring the impact of different drugs on the brain.
This interactive game you are about to play teaches you how different drugs affect the brain by allowing you to “reach” into a glass container full of laboratory mice under the effects of various drugs and pull them out for analysis.
- Break students into pairs or small groups and ask them to access the Mouse Party game from the University of Utah Genetic Science Learning Center (note: sound is required, headphones recommended).
- Ask students to select each of the mice one-by-one and drop them into the chair for analysis.
- Ask students to listen to the analysis of how the drug is impacting the mouse’s brain and click “Next” to hear all of the information.
- Have students fill out the Mouse Party student worksheet as the game tells them about the drug impacting each mouse.
EXPLAIN: What Do Drugs Do To The Brain?
The following information is teacher-facing and can be utilized to teach students new information in whatever format works best for you and your students.
Key Points:
- Some substances influence the brain and body by interfering with neurotransmitter signaling functions.
- Over time, a substance that overstimulates neural signaling can cause neurons to reduce their responsiveness, leading to tolerance of the drug.
- Other substances act by mimicking neurotransmitters, hormones, or other naturally occurring molecules.
- Substances that target components of the brain’s reward system are more likely to lead to addiction.
Disrupting Neurotransmitters At The Synapse
Some drugs that alter how the brain works do so by affecting the function of a particular neurotransmitter. (See more about neurotransmitters and their roles in Unit 1, Lesson 3.) For example, many drugs that are used to treat anxiety and depression are selective serotonin reuptake inhibitors (SSRIs), which cause serotonin to hang around longer in the space between neurons. This lets the transmitter have a bigger impact on the postsynaptic cell, which can promote relaxation and calmness in certain brain circuits that use serotonin. Another example is caffeine, which interferes with the signaling of the neurotransmitter epinephrine (also known as adrenaline), giving coffee drinkers a boost in attention and energy.
Example: Disrupting Dopamine
Many substances that can lead to addiction alter the neurotransmission of dopamine, since dopamine is involved in feelings of reward. A set of neurons in the brainstem that produce dopamine send their axons right to one of the most important reward centers of the brain, the nucleus accumbens. As illustrated in the figure below, typically dopamine (1) attaches to its receptor (2) on the postsynaptic cell (3) to activate a signal and then is recycled by its transporter (4) back into the presynaptic cell (5). Some drugs like cocaine, however, block the dopamine transporter from working (6) while others like methamphetamine temporarily reverse the direction of the transport (7). Either way, these drugs keep more dopamine in the synapse, which can lead to the feeling of reward, as the main reward networks of the brain contain dopamine synapses. This creates the “high” experienced in drug use; the pleasurable feeling of unusually high neurotransmitter activity in the brain’s reward centers. If repeated for a long time, this process can eventually lead to overstimulation of the postsynaptic cells in those brain areas, which may then remove some dopamine receptors in an effort to protect cells from toxic overload. When this happens, normal levels of dopamine (i.e., those produced by normal rewards) no longer have as much impact and those rewards feel smaller by comparison. Even the usual level of the drug doesn’t produce a “high” anymore (known as tolerance), causing a person to seek out a higher dose of the drug and making it harder to quit. Eventually, many individuals continue taking the drug they are addicted to not to get high, but just to feel normal.
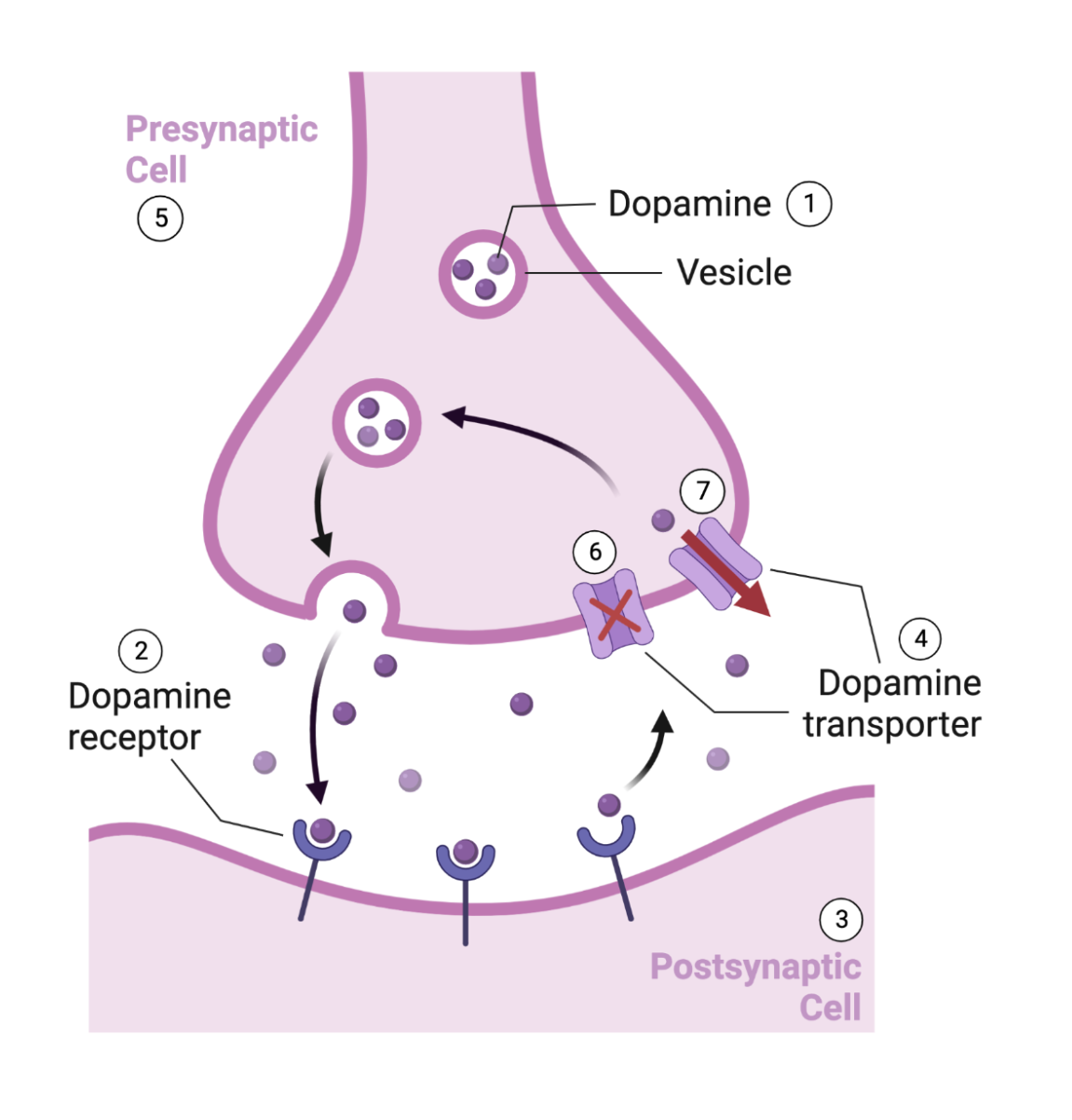
Alteration in the neurotransmission of dopamine is one main theory on the mechanism of addiction. Image credit: BioRender.com
Other Mechanisms of Action
Other common substances impact the body through different mechanisms:
- Opioids: Our bodies have naturally occurring molecules called endorphins that relieve pain and promote a sense of well-being (such as a “runner’s high”). Opioid medications used as painkillers mimic endorphins and bind to their receptors. However, stronger opioids like heroin have an even bigger impact, creating an unusually strong reward, creating the “high” that a person may experience.
- Hallucinogens: Many hallucinogenic substances mimic the neurotransmitter serotonin. These drugs bind very strongly to one particular type of serotonin receptor that can be found in many types of neurons. This produces changes in patterns of neural activity across the entire brain, making it less synchronized and creating the hallucinations that the drugs are known for. Conversely, most antipsychotic medications (often used as a treatment for schizophrenia) block or reduce the activity of certain serotonin receptors. Due to some hallucinogens (like psilocybin, the main chemical in “magic mushrooms”) impact on serotonin being somewhat similar to the mechanism of SSRIs, scientists and mental health professors are exploring using low, controlled doses of these drugs as a new classic of medications for anxiety and depression.
- Marijuana: Marijuana mimics naturally occurring molecules called endocannabinoids which have a range of roles, including regulating appetite, memory, emotional processing, and sleep. Use of the drug can impact all of these functions—while lower doses can be used medicinally to offset pain and nausea, higher doses may produce a hallucinogenic effect. Since hallucinogens and marijuana impact the reward pathway less directly than opioids or stimulants like amphetamine or cocaine, they tend to be much lower risk for substance use disorder.
- Alcohol: Alcohol is an example of a substance that impacts multiple systems in the brain and body. Its relaxing sedative effect, in particular, is due to the mechanism by which it both enhances the effect of GABA, the most common inhibitory neurotransmitter in the brain, and reduces the impact of glutamate, the most common excitatory molecule. Refer to Unit 1, Lesson 3 for more details about common neurotransmitters.
Additional Resources
- Disrupting Neurotransmitter Pathways
- The Genetics Science Learning Center at the University of Utah has many resources about the science of addiction.
- This video gives a good overview of how drugs and medications influence brain function, including a brief review of neuronal structure and neurotransmission. (TED-Ed)
- Example: Disrupting Dopamine
- This video explains the brain’s reward system and how dopamine signaling gets hijacked by addictive substances. (Yale Medicine)
- This article describes the distinction between drug tolerance, dependence, and addiction. (Healthline)
- Other Mechanisms of Action
- The National Institute on Drug Abuse (NIDA) has a website summarizing the health effects of many commonly used substances.
- NIDA’s DrugFacts publications also offer more comprehensive information about individual drugs.
ELABORATE: Neurotransmission Game Take 2! (30 min)
Revisit the Neurotransmission Game from Unit 1, Lesson 3 to demonstrate the different components involved in neurotransmission and see how this system is disrupted by commonly misused drugs like cocaine.
Follow the steps below:
- Break students into teams of 7-8
- Assign students in each team to the following roles:
- Presynaptic action potential (1 per team)
- Neurotransmitter vesicle (1 per team)
- Receptors (2 per team)
- Second messengers (2 per team)
- Transporters (1 per team)
- Cocaine (1 per team but not on all teams)
- Each team forms a line.
- Have the “presynaptic action potential” student stand a short distance away from the rest of the line.
- Say “go” to start the game. The presynaptic action potential student should run down and tag the neurotransmitter vesicle, then return to their starting position.
- When tagged by the action potentials, the vesicles throw a “neurotransmitter” (ping pong ball) across a gap to the receptors who catch it in their hands, a plastic cup, bowl, or large spoon (depending on how difficult you want to make the game).
- Once they’ve caught the ball, the receptor tags the second messenger students (who are standing right by them). The second messengers run over to the whiteboard and tally a point for their team to show depolarization. They then run back and tag the receptor.
- Once the receptor is tagged, the procedure differs between groups with and without a player acting as cocaine:
- In the groups WITHOUT cocaine: After the receptor is tagged, they throw the ball to the transporter, who catches and gives the ball back to the vesicle.
- Once the vesicle has the ball again, the presynaptic action potential can restart the process.
- In the groups with WITH cocaine: After the receptor is tagged, they throw the ball to the transporter, but cocaine stands in front of them and catches the call instead.
- Cocaine then throws it back directly to the receptor, who tries to catch it. The receptor and cocaine can throw it back and forth up to three times, triggering the second messengers again each time.
- Meanwhile, the presynaptic action potential can restart the process with a new ball, even as the old one is still being used by the receptor. This means that the receptor must pay attention to and catch balls from both the student playing cocaine and the student playing the vesicle.
- For all teams: If a receptor drops a ball, it is out of play. The transporter must kick the ball and return it to the vesicle to restart. The receptor cannot pick up any dropped balls, as receptors are bound to the cell membrane.
Once a team has tallied 10 points on the board, they have fired an action potential in the postsynaptic neuron and they win.
- In the groups WITHOUT cocaine: After the receptor is tagged, they throw the ball to the transporter, who catches and gives the ball back to the vesicle.
- After completing the game ask students to reflect on the following questions:
- Compare how this process looks different with and without the cocaine:
- What aspects of the process have changed when cocaine is involved?
- How does cocaine impact what the receptors do? How might this impact the receptors and the postsynaptic cell overall?
- Compare how this process looks different with and without the cocaine:
Lesson 3: Treatment & Policies for Substance Use
Objective: Students will learn about the currently available treatments for substance use disorders and how they are part of a changing landscape of social policies affecting youth.
ENGAGE/HOOK: Drug Testing in Schools (10 min)
Introduce the lesson by explaining the background information below:
The Butler Area School District in western Pennsylvania recently discussed updating its random drug testing policy in schools.
- Show students this video or read the accompanying article about Butler’s drug testing policies from a local news channel.
- Ask students to discuss the following questions after the video:
- Under the current policy, which students are subject to testing? What are the consequences for someone who tests positive?
- What are the policy changes being considered? Why?
- How does this policy compare to your own school?
- Do you think it is reasonable to conduct random drug tests among certain students? Why or why not?
EXPLORE: Opioid Treatment Simulation (30 min)
Explain the background information below to students to frame the following activity:
The University of Pittsburgh Public Health Dynamics Laboratory has developed a simulation for modeling the dynamics of opioid use disorder and overdose over a five year period of time (2020-2024) in specific counties in the U.S. The simulation looks at the impact of both naloxone (an emergency treatment for opioid overdose to prevent death, also known as Narcan) and buprenorphine (a prescribed medication for opioid use disorder that physicians use to help people addicted to many substances reduce their dependence on drugs). This kind of modeling is important because some people (including some politicians and officials) have discouraged use of naloxone out of worry that it promotes further drug use.
Pose the following question to students to consider as they complete the activity below:
- How does the availability of naloxone and buprenorphine affect the number of people in the county living with opioid use disorder (OUD) and the number of overdose deaths?
- Do you think the availability of naloxone promotes greater drug use (as some people have argued)?
- Have students go to the Opioid Treatment simulation website.
- Ask students to complete the steps outlined in the Opioid Treatment Simulation student worksheet as they investigate the website.
- Assign students in pairs to choose a county.
- Make sure at least one group chooses your own state/county if it is available.
- Have other groups model different state counties for comparison.
- In each group, one student will analyze numbers of OUD cases while the other will analyze the number of overdose deaths.
- After students complete the worksheet, have them complete the following discussion questions independently:
- What change do you observe as you increase the availability of naloxone?
- How does this compare to increasing the availability of buprenorphine? Of both naloxone and buprenorphine?
- How do different counties compare?
- What strategy would you recommend to county health officials?
- What might be some potential barriers to enacting this strategy in a county?
- Optional: Have students plot the data from their worksheets and create a line graph showing the change in either OUD cases or overdose deaths as they increase the availability of naloxone, buprenorphine, or both. Compare to other groups to see if anything is unique or the same patterns are seen. Some teachers may wish to complete this activity with a letter writing campaign to local officials.
EXPLAIN: Treatments, Policy Choices, and Societal Implications
The following information is teacher-facing and can be utilized to teach students new information in whatever format works best for you and your students.
Key points:
- Treatment for addiction can involve behavioral intervention and/or medical intervention.
- Changes in brain structure and function due to substance use increase the risk of relapse, but can also be reversed in long-term recovery.
- Effective education and healthcare for substance use involve long-term, holistic approaches that integrate scientific information with resources for ongoing support.
Treating Substance Use Disorders
Different strategies of treatment are useful at different stages of recovery. Naloxone is a medication that can be easily and quickly administered in emergency opioid overdose situations to block receptors and reverse the effects of other opioids, saving lives. Other medications commonly prescribed for treating opioid use disorders include buprenorphine, methadone, and naltrexone. Methadone activates the same receptors in the brain that opioids do, but in a slower, controlled manner and at a lower level, helping patients avoid withdrawal symptoms. Buprenorphine also activates the opioid receptors, but to a lesser extent. Naltrexone is similar to naloxone, in that it blocks the opioid receptors in the brain and prevents opioids from binding to them. However, naltrexone is taken orally (as opposed to naloxone, which is injected) and reduces the impact of opioids over a longer period of time (as opposed to quickly preventing overdose deaths).
In addition to medical treatments, behavioral therapies can support long term changes in attitudes and coping strategies to help stay in treatment and prevent relapse. There is some recent evidence that compounds derived from cannabis or psychedelics could also help manage substance use disorders and addiction, although their mechanisms of action are not well understood.
Detoxification, Relapse, and the Brain
Prolonged substance use can disrupt the normal functioning of neurotransmitters and lead to structural and functional changes in the brain. During detoxification, the brain must readjust to functioning without the drug, sometimes resulting in symptoms of withdrawal. Withdrawal symptoms can vary depending on the specific substance but may include both physical (such as fatigue, sweating, muscle pain, tremors, nausea, and seizure) and psychological symptoms, (such as paranoia, anxiety, confusion, and agitation). Medication can help manage both these types of effects. Changes in the brain due to substance use also help us understand why relapse is so common. Over time, the brain has created powerful associations between the drug and certain cues or triggers and frequently appeared during drug use. Exposure to these triggers reactivates the reward system and generates intense cravings for the substance. Chronic substance use also influences behavior because of its effects on regions of the brain involved with reward, decision making, stress response, and memory. Luckily, neuroplasticity means that the brain can continue to change during recovery! Research has shown that decreases in brain function can improve and even reverse after months of abstinence.
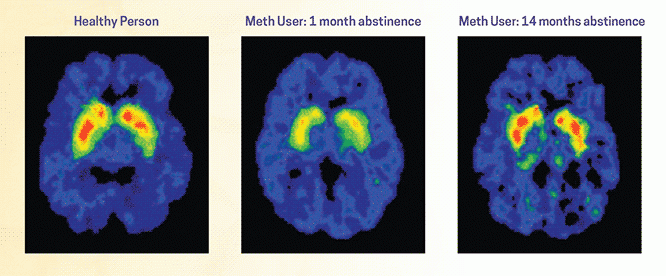
PET scans show that compared to a healthy person (left), dopamine signaling in the brain is significantly lower after methamphetamine use (middle), but can rebound after a long abstinence (right). Image credit: Journal of Neuroscience, 2001, 21(23):9414-9418.
New Approaches for Education & Health Policy
In the 1980s, youth education programs around substance use and addiction were focused on the idea of “just say no.” But a decade later, research showed that this approach had no effect on students’ choices about using alcohol and other substances. Today, evidence suggests that more effective prevention programs involve not just information (including neuroscience!) but also skills development, rules and enforcement strategies, and access to support services. Healthcare for substance use disorders has also evolved based on new evidence from neuroscience and other fields. Based on the brain changes underlying detoxification and relapse, there is more support for medical treatments that approach these disorders as chronic health conditions rather than a one-time cure, while “parity” laws require insurance coverage for substance use disorders to be comparable for other types of medical or surgical treatment.
Additional Resources
- Treating Substance Use Disorders
- This video gives a good overview of different medications used to treat substance use disorders and how they work. (National Institutes of Health)
- The National Institute on Drug Abuse (NIDA) has an overview of types of treatments for addiction and paths to recovery.
- This 2023 article discusses recent research on psychedelics as treatment for substance use disorders. (Los Angeles Times)
- This 2019 interview with scientist Yasmin Hurd highlights the opportunities and challenges of studying cannabinoid compounds for treating substance use disorders. (Nature)
- Detoxification, Relapse, and the Brain
- This brief article describes the causes of withdrawal after substance use. (BrainFacts.org)
- This website has a good overview of opioid withdrawal symptoms and treatment. (Healthline)
- This short video is a good overview of the signs of substance use relapse and three stages: emotional, mental, and physical. (GoodRx)
- This article summarizes research to understand how social connections can reduce cravings and the likelihood of relapse. (BrainFacts.org)
- New Perspectives on Education & Policy
- This website is a good summary of current evidence-based approaches to prevention education. (Youth.gov)
- The Illicit Project, an experimental substance education program being tested in Australian schools, includes neuroscience along with strategies for mental health and well-being.
- This resource describes a chronic care plan for managing a substance use disorder, reflecting new approaches to addiction medicine. (Addiction Policy Forum)
ELABORATE: Should Students Be Trained to Use Narcan? (30 min)
Explain the background information below to students to frame the following activity:
A school district in Virginia has recently started allowing students to carry Narcan. The activity below will help us unpack this decision:
- Have students read or listen to a news report from National Public Radio about the Virginia school district allowing students to carry Narcan to respond to drug overdoses.
- Guide students through a Question Formulation process to reflect on the story and identify questions that would be important to answer before implementing a similar policy in your school:
- Brainstorm questions:
- Ask as many questions as you can.
- Do not stop to discuss, judge, or answer the questions.
- Write down every question exactly as it is stated.
- Change any statement into a question.
- Identify open- and closed-ended questions
- Prioritize three questions that would be most important for considering a Narcan policy for your school, and discuss the rationale for their choices.
- Brainstorm questions:
For more information about the Neuroscience & Society Curriculum, please contact neuroscience@fi.edu.
Neuroscience & Society Curriculum
Launch Lesson • Unit 1: Neurons and Anatomy • Unit 2: Education and Development • Unit 3: Current Methods in Neuroscience • Unit 4: Mental Health and Mental Health Conditions • Unit 5: Drugs and Addiction • Unit 6: Law and Criminology • Unit 7: Future Technologies

This project was supported by funding from the National Institutes of Health Blueprint for Neuroscience Research under grant #R25DA033023 and additional funding from the Dana Foundation. Its content is solely the responsibility of the authors and does not necessarily represent the official views of NIH or the Dana Foundation.